Indications for a paracentesis
Indications for a paracentesis
– Evaluate etiology of new- onset ascites
– Rule out spontaneous bacterial peritonitis
– Follow-up of therapy for spontaneous bacterial peritonitis
– Respiratory compromise in patients with massive ascites
– Management of refractory, cirrhotic ascites
– Adjunctive management of hepatorenal syndrome
Contraindications for a paracentesis
– Acute abdomen requiring exploratory surgery
– Infected abdominal wall at the entry site
– Uncooperative patient
– DIC or significant fibrinolysis
– Severe bowel distension or bowel obstruction
– Multiple prior abdominal surgeries
– Pregnancy
– INR > 5 (INR > 2.5 on warfarin)
– Coagulopathy with PTT 1.5x upper limit of normal
– Incidence of severe hemorrhage 0.2%(N= 4,500 paracenteses)
– Bleeding is reduced with ultrasound- guidance
– Thrombocytopenia (Platelets<25k)
– Use of DOAC or fondaparinux
Complications of a paracentesis
– Bowel or bladder perforation
– Hemoperitoneum (0.2%)
– Hypotension with large volume paracentesis
– Hepatorenal syndrome
– Persistent ascitic fluid leak (1 % risk)
-Stitch vs ostomy bag vs dermabond 1 mL injected 1 cm deep
– Metastatic seeding of needle tract (rare)
– Soft tissue infection at puncture site
– Abdominal wall hematoma
Equipment for a paracentesis
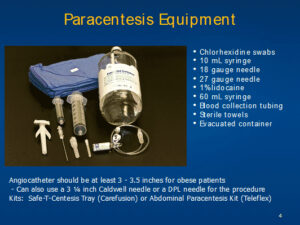
Angiocatheter should be at least 3 – 3.5 inches for obese patients
– Can also use a 3 ¼ inch Caldwell needle or a DPL needle for the procedure
Kits: Safe-T-Centesis Tray (Carefusion) or Abdominal Paracentesis Kit (Teleflex)
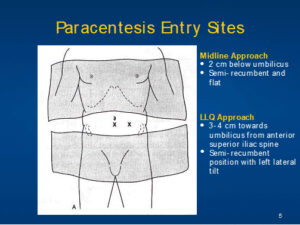
Proper positioning and technique for a paracentesis
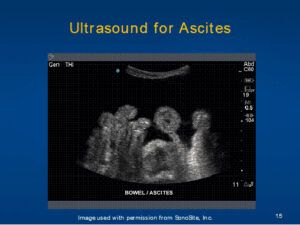
Ultrasound-directed paracentesis
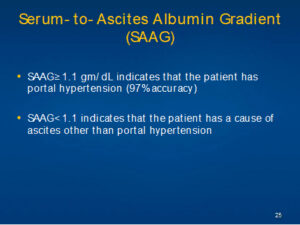
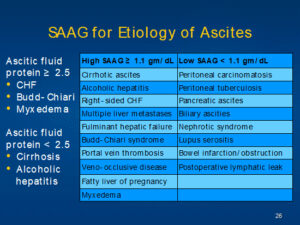
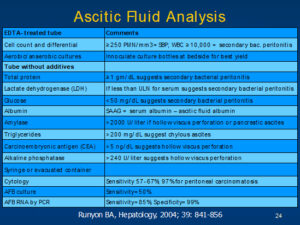
Ascitic fluid analysis
Coding for a paracentesis
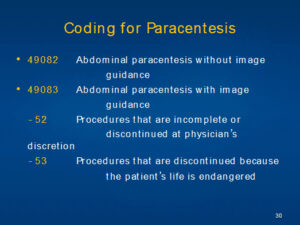
– 52 Procedures that are incomplete or discontinued at physician’s discretion
– 53 Procedures that are discontinued because the patient’s life is endangered