Indications for a diagnostic lumbar puncture
Indications for a diagnostic lumbar puncture
– RBC in CNS can mean a traumatic tap, but expect the RBC to clear
from tubes 1-4
– Xanthrochromia (pink or yellow tint) represents hemoglobin
breakdown after two hours.
– Elevated opening pressure
– Exceedingly rare if third-generation head CT scan negative
– Suspected meningeal carcinomatosis
– Pseudotumor cerebri
– Tuberculous meningitis
– CNS syphillis
– CNS vasculitis (very rare)
– Multiple sclerosis
– Guillain Barre syndrome
– Transverse myelitis
Indications for a therapeutic lumbar puncture
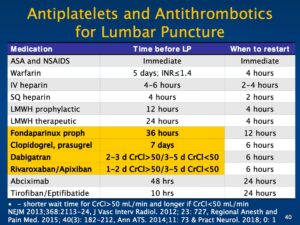
Contraindications for a lumbar puncture
– Now use Platelets <50,000
– Active anticoagulation or recent receipt of antithrombotics or thienopyridines
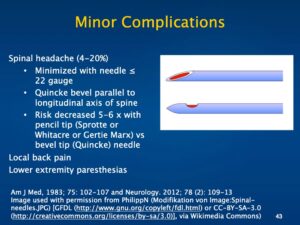
Complications of a lumbar puncture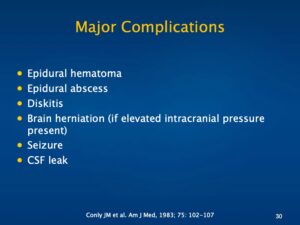
Equipment for a lumbar puncture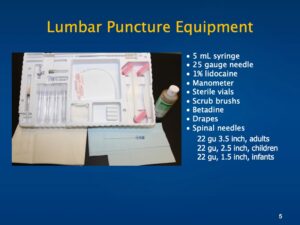
22 gu 3.5 inch, adults
22 gu, 2.5 inch, children
22 gu, 1.5 inch, infants
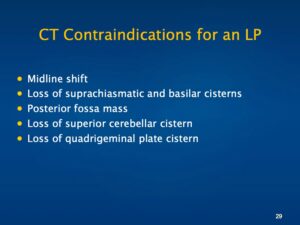
When to get a CT scan of the head prior to a lumbar puncture
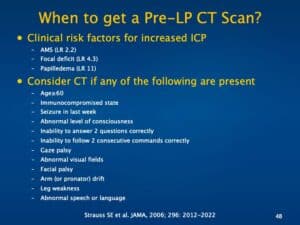
– AMS (LR 2.2)
– Focal deficit (LR 4.3)
– Papilledema (LR 11)
– Age≥60
– Immunocompromised state
– Seizure in last week
– Abnormal level of consciousness
– Inability to answer 2 questions correctly
– Inability to follow 2 consecutive commands correctly
– Gaze palsy
– Abnormal visual fields
– Facial palsy
– Arm (or pronator) drift
– Leg weakness
– Abnormal speech or language
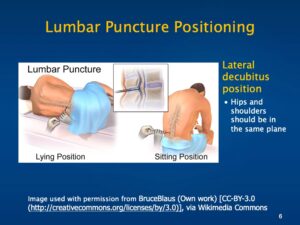
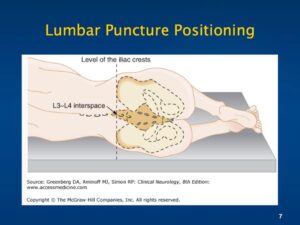
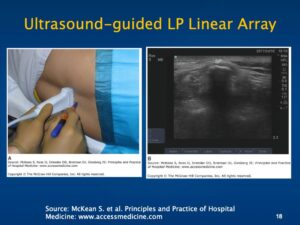
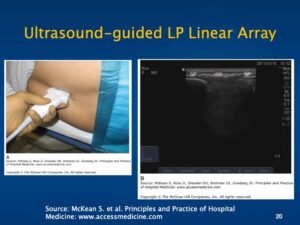
Proper positioning and technique for a lumbar puncture
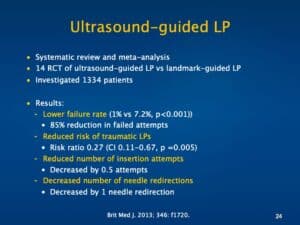
– Lower failure rate (1% vs 7.2%, p<0.001))
– Reduced risk of traumatic LPs
– Reduced number of insertion attempts
– Decreased number of needle redirections
Cerebrospinal fluid analysis
– Cell count with differential
– Culture and gram stain
– Glucose and protein
– Infectious studies: VDRL, cocci titer, AFB RNA by PCR, encephalitis
panel, India ink, cryptococcal antigen, adenosine deaminase level
(for Tb), lactate level, HSV RNA by PCR, VZV RNA by PCR
– Multiple sclerosis: Oligoclonal bands, IgG index, myelin basic
protein
– Cytology
– ACE level
Coding for a lumbar puncture